What are the causes of Thrombophilia?
When there is bleeding or an injury to a blood vessel, the blood clotting process occurs naturally. Blood clots are formed to stop excess blood from leaking, and once the injury is healed, the blood clot will dissolve. However, people with thrombophilia have an altered blood-clotting cascade, leading to an increase in blood hypercoagulability and risk of thrombosis.
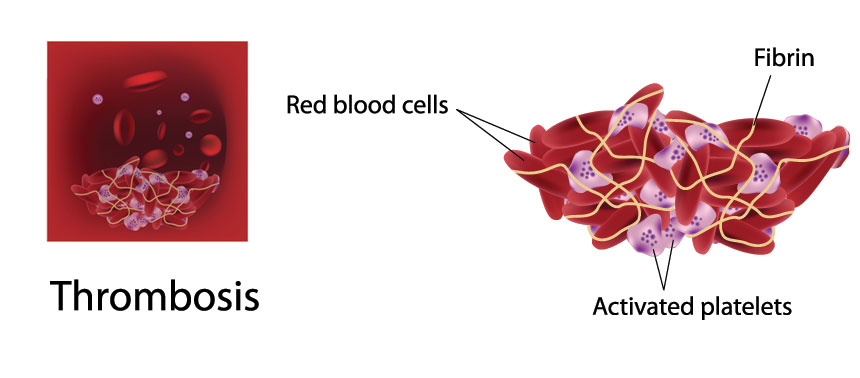
Under normal circumstances, the blood-clotting cascade starts when there is an injury to the blood vessel. The platelets in the blood attach to the walls of the blood vessels, followed by disintegration and release of an enzyme called thromboplastin. This enzyme is used for converting prothrombin in the blood plasma into thrombin with the help of calcium. Thrombin, in turn, is used for converting fibrinogen to fibrin, which forms an insoluble, net-like covering over the damaged blood vessel. The fibrin network then traps the red blood cells, white blood cells and platelets as the blood flows through, and forms a clot that acts to seal the endothelium of the blood vessel completely. There are many enzymes and cofactors that take part in this clotting cascade, and mutations in these genes cause an upset in the clotting cascade.
Thrombophilia refers to a group of conditions where there is a higher tendency for blood to form abnormal clots, leading to an increased risk of developing thrombosis. Inherited thrombophilia and acquired thrombophilia are the two general types of thrombophilia.
Inherited Thrombophilia
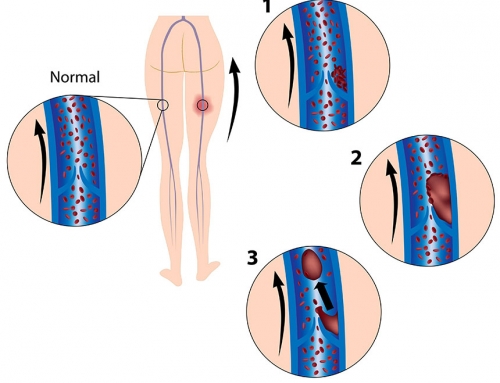
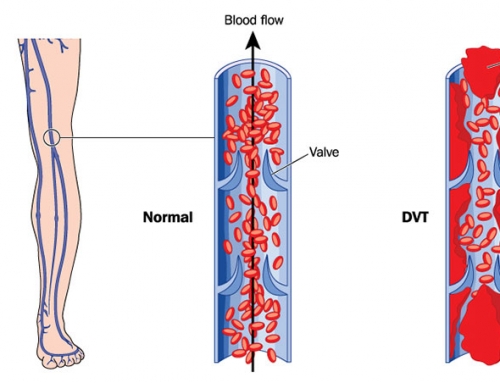
Inherited thrombophilia is caused by genetic mutations that affect the blood-clotting cascade, leading to thrombosis and other complications. Thrombosis is mainly caused by damage to the endothelial cells of the blood vessels, blood hypercoagulability and slow flow of blood (blood stasis). Different genetic mutations affect the clotting cascade in various ways, and are described as different types of inherited thrombophilia. Four of the most common changes leading to an increased blood clotting risk are Factor V Leiden, Prothrombin 20210 and deficient Protein C and MTHFR activity.
Factor V Leiden:
The Factor V protein is responsible for the activation of prothrombin to form a clot. Normally Factor V is controlled by Protein C and Protein S to prevent abnormal blood clotting. However, a mutation in the Factor V gene (F5), known as the Factor V Leiden mutation, reduces the inhibition by Protein C and Protein S. This prolongs the clotting process and increases the risk of abnormal blood clots forming in a vein.
Prothrombin 20210:
Prothrombin acts as a clotting factor in the cascade. A mutation in this gene (20210G>A) leads to hypercoagulability of blood and an increased risk of forming a blood clot.
Protein C deficiency:
Protein C is a key component responsible for inhibiting blood coagulation in the clotting cascade. A deficiency in protein C results in less inhibition of clotting factors, leading to a prolonged clotting process and an increased risk of forming blood clots.
MTHFR deficiency:
The methylenetetrahydrofolate reductase (MTHFR) enzyme helps process Vitamin B9, which is required in the process of converting homocysteine to methionine. Changes in the MTHFR gene, cause the enzyme to not be as efficient at processing Vitamin B9/folate and an excess of homocysteine accumulates, leading to abnormal blood clotting.
Acquired Thrombophilia
Acquired thrombophilia is caused by a compromised immune system or existing medical conditions. The most commonly observed acquired thrombophilia is antiphospholipid syndrome (APS). The compromised immune system resulting from this syndrome, causes antibodies to circulate abnormally in the blood, leading to blood clots forming in arteries, veins and small blood vessels. Other medical conditions such as platelet, bone marrow and kidney disorders, inflammatory bowel disease and cancer may also increase the risk of a blood clot.
Mixed Thrombophilia
Mixed thrombophilia is caused by both genetic and non-genetic causes. The most commonly observed mixed thrombophilia is hyperhomocysteinaemia. This condition can be caused by a mutation in the MTHFR gene combined with a dietary cause, such as over consumption of caffeine, or reduced intake of folic acid, vitamin B6 and B12. This condition may also result from renal impairment and hypothyroidism.
References:
Angelini A, Febbo CD, Baccante G, Nisio MD, Ilio CD, Cuccurullo F, Porreca E (2003). Identification of Three Genetic Risk Factors for Venous Thrombosis Using a Multiplex Allele-Specific PCR Assay: Comparison of Conventional and New Alternative Methods for the Preparation of DNA from Clinical Samples. Journal of Thrombosis and Thrombolysis. 16(3): 189-193.
den Heijer M, Lewington S, Clarke R (2005). Homocysteine, MTHFR and risk of venous thrombosis: a meta-analysis of published epidemiological studies. J Thromb Haemost. 3: 292-9.
Gatt A, Makris M. Hyperhomocysteinemia and venous thrombosis (2007). Semin Hematol. 44(2): 70-6.
Gohil R, Peck G, Sharma P (2009). The genetics of venous thromboembolism. A meta-analysis involving approximately 120,000 cases and 180,000 controls. Thromb Haemost.102(2): 360-70.
Kujovich JL (2011). Factor V Leiden Thrombophilia. Genetics in Medicine. 13: 1-16. doi:10.1097/GIM.0b013e3181faa0f2
McGlennen RC, Key NS (2002). Clinical and laboratory management of the prothrombin G20210A mutation. Arch Pathol Lab Med. 126(11): 1319-25.
Press RD, Bauer KA, Kujovich JL, Heit JA (2002) Clinical utility of factor V leiden (R506Q) testing for the diagnosis and management of thromboembolic disorders. Arch Pathol Lab Med. 126(11): 1304-18.
White RH (2003). The epidemiology of venous thromboembolism. Circulation. 107(23 Suppl 1): I4-I8.
DNA In the News2017-04-06T20:02:09+00:00