Who should be considered for Thrombophilia diagnosis and how is it done?

People with inherited or acquired thrombophilia are normally asymptomatic until blood clots forms. Therefore, if there is any family history, personal medical history, or pregnancy problems suggestive of thrombophilia, these people should be considered for diagnosis of thrombophilia.
Family history
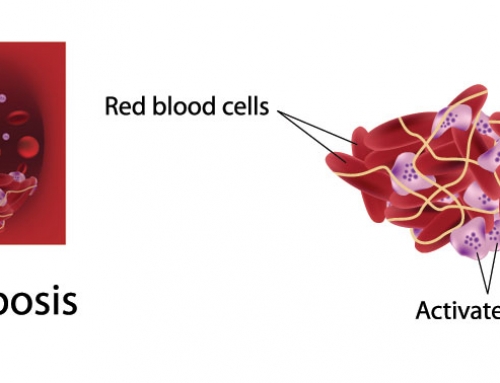
Thrombosis
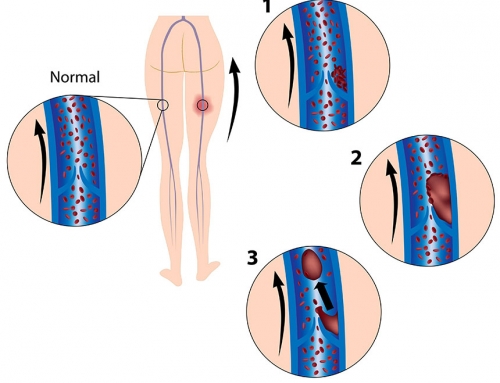
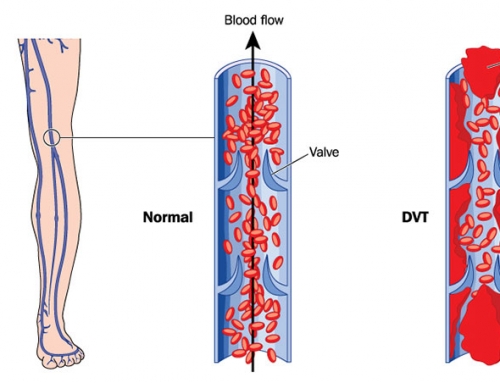
Deep Vein Thrombosis (DVT)
Pulmonary Embolism (PE)
Inherited thrombophilia
Personal medical history
Thrombosis at a young age, <40 yrs old
Frequent episodes of DVT, PE or thrombophlebitis (inflamed veins)
Develop skin necrosis (skin patch loss due to blood clots underneath the skin) due to medicines such as warfarin
Pregnancy
Recurrent pregnancy loss
Miscarriage
Fetal death
Neonatal babies with purpura fulminans (homozygous Protein C and Protein S deficiencies)
Neonatal babies with thrombosis
Thrombophilia is diagnosed by blood and genetic analyses. Blood coagulation screening tests, such as the APC resistance assay, indicate whether or not a patient is at an increased risk of abnormal blood clotting. Blood analyses can only be conducted when the patient is not taking any anticoagulant medication and is not currently suffering from any blood clotting problems or during pregnancy, as each of these factors influence the coagulation screening result. Specific genetic mutations in three genes (F5, F2 and MTHFR) significantly increase the risk of thrombophilia. A genetic analysis can be conducted at any point (even while on anticoagulant medication or prior to any symptoms appearing) to determine if an individual carries one or more of the genetic changes associated with thrombophilia.
References:
Gatt A, Makris M. Hyperhomocysteinemia and venous thrombosis (2007). Semin Hematol. 44(2): 70-6.
Kujovich JL (2011). Factor V Leiden Thrombophilia. Genetics in Medicine. 13: 1-16.
Press RD, Bauer KA, Kujovich JL, Heit JA (2002) Clinical utility of factor V leiden (R506Q) testing for the diagnosis and management of thromboembolic disorders. Arch Pathol Lab Med. 126(11): 1304-18.
DNA In the News2017-04-06T20:05:36+00:00